What Bloodwork Should You Monitor on GLP-1? A Practical Checklist
TL;DR
- Bloodwork on semaglutide is not about whether the drug is safe: for most people it is well tolerated. It is about monitoring the right markers at the right intervals instead of monitoring nothing.
- Standard telehealth program monitoring is usually a minimum-safety floor, not optimization. Knowing what to ask for, and why, is on you: not the program.
- The checklist covers four buckets: metabolic baseline, organ function, thyroid (with calibrated risk framing, not scare copy), and the markers that tell you the drug is doing what you want for body composition.
- One panel most guides skip: testosterone. For any man in a significant caloric deficit, the hormonal picture shifts, and the direction is worth tracking.
If you want to know what bloodwork to monitor on semaglutide, the useful answer is not a generic lab list: it is a monitoring protocol with intervals and reasons attached. GLP-1 medications are well tolerated in most users, which is exactly why the failure mode here is not over-monitoring; it is monitoring nothing because the program said it would handle things. The drug is doing real metabolic work in your body. Holding a baseline and rechecking the right markers tells you two things at once: that nothing is quietly going wrong, and that the intervention is actually moving the numbers you care about.
Here is the checklist I would want if I were starting again, organized by what each marker tells you.
Download the free GLP-1 Starter Framework, the three-lever system for losing fat without losing muscle.
Why the Standard Telehealth Protocol Isn’t Enough
This is an observation about scope, not a criticism of any specific program. A telehealth GLP-1 program’s monitoring is built to clear a safety bar: confirm you are an appropriate candidate, catch the rare serious problem, keep the prescription compliant. That floor is reasonable. What it does not do is tell you whether the drug is doing what you want it to do for your body composition, or give you the baseline you would need to interpret a change six months from now.
That data gap is yours to close. The program is optimizing for safe prescribing at scale. You are optimizing for a specific outcome (losing fat while holding muscle), and that requires markers and intervals the standard protocol was never designed to provide.
The Core Bloodwork Checklist
Metabolic markers
Fasting glucose, HbA1c, fasting insulin, and HOMA-IR (calculated from glucose and insulin) are the core metabolic panel. Fasting glucose and HbA1c show your average glucose control; fasting insulin and HOMA-IR show insulin sensitivity, which is often where GLP-1 produces its most meaningful improvement. These are the numbers most likely to move in a direction you will be glad you documented. They also tie directly to the glucose-dependent mechanism that makes hypoglycemia low-risk as monotherapy, and why glucose markers are still worth tracking.
Lipid panel
GLP-1 medications tend to improve lipids. A baseline plus a 12-week recheck gives you a real trajectory rather than a single snapshot. Watch the full panel (total cholesterol, LDL, HDL, triglycerides), with particular attention to triglycerides, which often respond well to the fat loss and insulin-sensitivity improvements.
Liver function
ALT and AST track liver status. In people with fatty liver disease, semaglutide has been shown to reduce liver fat, so a baseline matters for two reasons: it helps catch anything unexpected, and it gives you a comparison point if elevated liver markers improve as visceral and liver fat come down. For a lot of men carrying excess visceral and liver fat, this is one of the panels that may improve visibly.
Kidney function
eGFR and creatinine cover kidney function. This is relevant in a caloric deficit context and worth a baseline. Dehydration during the early weeks (when nausea and reduced intake are common) can transiently affect these markers, which is another reason a clean starting baseline is useful for interpreting later results.
Thyroid: with calibrated risk framing
This is the panel most articles get wrong by overstating it. GLP-1 drugs carry a boxed warning for medullary thyroid carcinoma (MTC), and that warning traces to rodent studies where GLP-1 receptor activation caused thyroid C-cell tumors. The honest context: rodents have a far higher density of GLP-1 receptors on thyroid C-cells than humans do, and a causal link to MTC has not been established in humans (FDA prescribing information). The drugs are contraindicated if you have a personal or family history of MTC or the genetic syndrome MEN2: that contraindication is firm. For everyone else, the calibrated read is that the risk signal is real enough to take seriously and respect the contraindication, but not the looming threat that scare copy implies. A baseline TSH is reasonable. If you have any thyroid history, that belongs in the conversation with your prescriber before starting. (This reflects the current FDA framing; confirm against the prescribing information for your specific drug, since labeling is updated periodically.)
Testosterone and SHBG
This is the panel most male GLP-1 users should add and most guides omit. Significant fat loss changes the hormonal picture: less adipose tissue means less aromatase activity, which can shift the testosterone-to-estradiol balance. Tracking total and free testosterone, plus SHBG, tells you the direction your hormonal context is moving as your body composition changes. It is not about chasing a number: it is about not flying blind on a system that fat loss directly affects.
Timing: Before, During, and After
The protocol is simple; it just has to be specific:
- Baseline (before starting): the full panel: metabolic, lipid, liver, kidney, TSH, testosterone/SHBG. This is the comparison everything else gets measured against.
- 12 weeks: recheck metabolic markers and lipids to confirm the trajectory. This is early enough to catch a problem and late enough to show real movement.
- 6 months: a fuller recheck, including liver and kidney if anything looked off at baseline, plus testosterone if you are tracking the hormonal shift.
- Annually: the full panel again, as a standing baseline for the long run.
I ran a full panel before I started (metabolic markers, lipids, testosterone, liver function), and built a simple spreadsheet to track each value across time points. Those pre-start labs are the baseline I compare everything against, and the single most useful thing about them is that they exist; you cannot reconstruct a baseline after the fact. That is how I approached it, not monitoring advice: what you test and when is a decision for you and your physician.
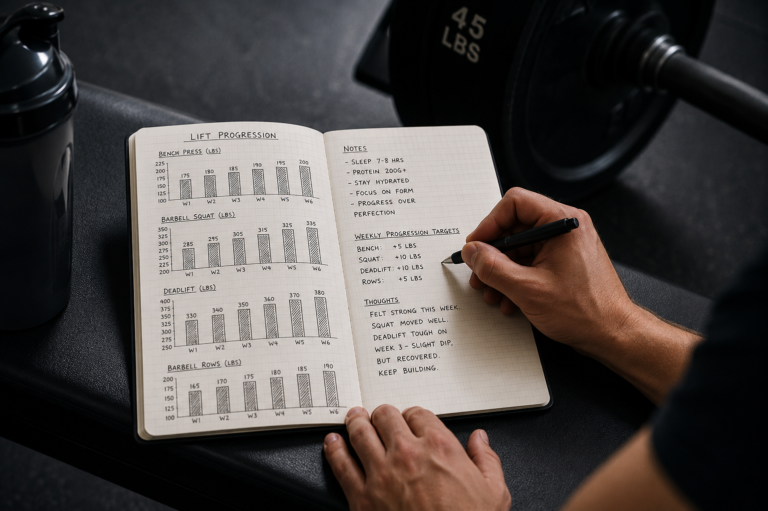
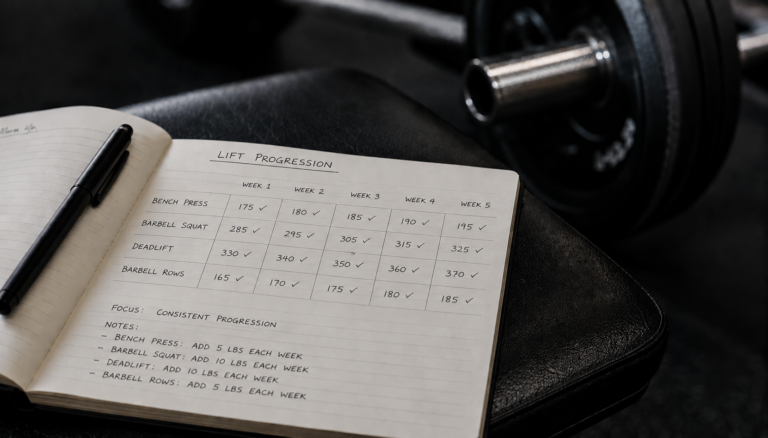
The Physical Performance Layer
Here is the limit of bloodwork: labs track metabolic function, but they do not track lean mass. You can have a flawless metabolic panel while quietly losing muscle, because no blood marker reports your lean mass directly. That is the blind spot the monitoring protocol has to cover with something other than a needle.
The physical layer means strength benchmarks (are your working weights holding or climbing?), circumference measurements (is your waist dropping while your arms and legs hold?), and a DEXA scan where you have access to one. Together they tell you what the bloodwork cannot: whether the weight you are losing is coming off fat or off your frame. This is exactly the gap the trial data exposes: what the STEP trial body composition data showed, and why lean mass tracking is the missing layer in most monitoring protocols. A dedicated article on building strength and circumference benchmarks into your monitoring is coming. For the full picture of how GLP-1 acts across every system you might be tracking, see the complete GLP-1 mechanism breakdown.
Download the free GLP-1 Starter Framework, the three-lever system for losing fat without losing muscle.
The GLP-1 & Body Composition guide ($7) covers what the trials measured, why lean mass tracking matters, and how to interpret body-composition markers alongside bloodwork.
FAQ
Do I need bloodwork before starting a GLP-1 medication?
A prescriber will typically check basic labs to confirm you are an appropriate candidate, but the minimum prescribing panel is narrower than what is useful for tracking your own outcomes. A fuller baseline (metabolic markers, lipids, liver, kidney, TSH, and testosterone for men) gives you the comparison point you will want later. You cannot reconstruct a baseline after you have started, so getting it before the first dose is the one timing decision that is genuinely one-way.
How often should I get labs checked while on Ozempic or Wegovy?
A reasonable rhythm is a full baseline before starting, a recheck of metabolic markers and lipids around 12 weeks, a fuller panel at 6 months, and an annual full panel after that. If your baseline showed anything elevated, such as liver enzymes, glucose, or lipids, your prescriber may want to recheck sooner. The intervals matter less than having a baseline and a consistent comparison; erratic, one-off labs tell you much less than a tracked series.
Does semaglutide actually cause thyroid cancer?
There is no established causal link to thyroid cancer in humans. The boxed warning comes from rodent studies where GLP-1 receptor activation caused thyroid C-cell tumors, and rodents have far more GLP-1 receptors on those cells than humans do. The drugs are contraindicated if you have a personal or family history of medullary thyroid carcinoma or MEN2. For everyone else, the risk signal is taken seriously without evidence of meaningful human risk. Discuss any thyroid history with your prescriber before starting.
Should I monitor testosterone levels while on GLP-1?
For men in a significant caloric deficit, it is worth doing. Fat loss reduces aromatase activity, which can shift your testosterone-to-estradiol balance, so the hormonal picture moves as your body composition changes. Tracking total and free testosterone plus SHBG at baseline and again as you lose fat shows you the direction. Sometimes fat loss improves the picture; sometimes it uncovers pre-existing low testosterone that excess body fat was masking. Either way, you want the data rather than a guess.
What blood markers indicate a problem with kidneys or liver on GLP-1?
For the kidneys, rising creatinine or a falling eGFR is the signal: though early-treatment dehydration from nausea and reduced intake can cause transient changes that resolve with rehydration. For the liver, rising ALT and AST would warrant attention, though GLP-1 drugs more often improve liver enzymes in people with fatty liver. Any persistent or significant abnormality is a conversation with your physician, not something to interpret or act on alone.
Nothing on this site constitutes medical advice. I’m not a physician, and this blog documents my own research and experience. Consult a qualified healthcare provider for decisions about medication, dosing, or treatment.
Ryan Mercer | MetabolicMale.com | ryanmercer@metabolicmale.com
References
- FDA prescribing information for semaglutide and tirzepatide products.
- Flint A et al. Aliment Pharmacol Ther, 2021.
- Wilding et al. Journal of the Endocrine Society, 2021.