Rate of Weight Loss on GLP-1: The Number Most Users Are Completely Ignoring
TL;DR
- Rate of weight loss on GLP-1 is the third lever, and the one almost nobody manages. How fast the scale drops largely decides whether you’re losing fat or muscle.
- Above roughly 1% of bodyweight per week, the body starts recruiting lean tissue because fat mobilization can’t keep pace with the energy demand.
- GLP-1 pushes many users past that line passively. The appetite suppression is strong enough to create steep deficits with no hunger signal to correct them.
- The target range is 0.5–1.0% per week. The tool to hold it is a deliberate caloric floor, tracked against a 7-day rolling average.
- When loss runs hot, add calories: protein first, then carbs, then fat. Never cut protein to hit a floor.
Most GLP-1 users track one number: scale weight. They watch it drop and read a fast drop as the drug working exactly as it should. What they’re not tracking is how fast that drop is happening, and the rate of weight loss on GLP-1 is one of the most important variables determining whether the loss comes from fat or from muscle.
This is the third of three levers that determine body composition. The other two (protein intake and resistance training) get more attention. Rate of loss is the one people are either not thinking about or actively celebrating getting wrong. If you’d rather have the management protocol than the full reasoning, the free GLP-1 Starter Framework builds it in.
Why Rate of Loss Determines What You Lose
Fat mobilization from adipose tissue has a ceiling. The body breaks down and oxidizes stored triglycerides at a rate set by lipolytic enzyme activity, fatty acid transport, and mitochondrial oxidation capacity. Below that ceiling, the caloric deficit is met predominantly from fat. Above it, the body increasingly recruits lean tissue, breaking down muscle protein through gluconeogenesis to meet energy demands fat oxidation can’t supply fast enough.
The rate of loss is the mechanism by which that ceiling gets breached.
The most-cited evidence comes from Garthe I et al. (Int J Sport Nutr Exerc Metab. 2011;21(2):97-104), comparing two loss rates in athletes, about 0.7% versus 1.4% of body weight per week. The slower group preserved significantly more lean mass and maintained better performance.
Population caveat, and it matters: Garthe studied elite athletes, not GLP-1 users or people with excess adiposity. The directional finding (faster loss drives greater lean catabolism) is supported by the broader weight loss literature, but the population differs from the typical GLP-1 user. Apply the principle; don’t port the numbers directly.
The target drawn from the broader literature: 0.5–1.0% of body weight per week. Below 0.5% and fat loss is very slow; above 1.0% and lean catabolism becomes a progressively larger fraction of the total.
What GLP-1 Does to Rate of Loss
GLP-1 receptor agonists suppress appetite centrally through hypothalamic satiety signaling, brainstem circuits, and mesolimbic food reward. The suppression can be powerful enough that users run large deficits with no hunger signal to correct the shortfall.
A reference point for GLP-1 loss rates comes from STEP 4: mean weight loss over the 20-week semaglutide run-in was 10.6% of body weight (Rubino D et al. JAMA. 2021;325:1414-1425), averaging roughly 0.5% per week across the full run-in. But loss on GLP-1 is front-loaded. Rates in the first four to eight weeks, when suppression is strongest and doses are escalating, run higher than the mean. The average masks early-phase rates that frequently exceed the target range.
Most people see fast loss and read it as the drug working as intended. I tracked my rate every week from the start, not because I wanted to slow down, but because I knew what fast loss costs in lean tissue. The goal wasn’t maximum weight loss. It was maximum fat loss. Those aren’t the same number, and on GLP-1 they can diverge sharply. What that divergence looks like in the trial data puts numbers on it.
How Most GLP-1 Users Think About This (And What’s Different)
The standard mental model: the scale drops, the drug is working, fast is better than slow.
The body composition model: a fast drop tells you the drug is working. It doesn’t tell you what the loss is made of. Fast loss unmanaged means a meaningful fraction of what you’re losing is lean tissue you’ll have to rebuild later.
The reframe isn’t “slow down.” It’s “manage your rate so what you’re losing is predominantly fat.”
How to Calculate and Manage Your Rate
All examples in pounds.
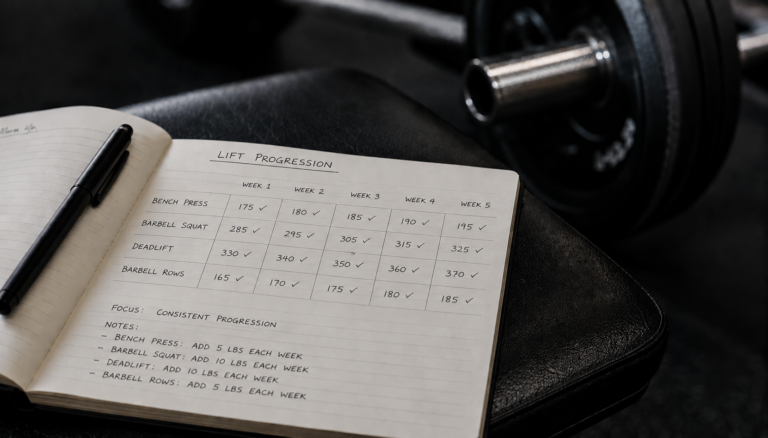
Step 1: Calculate the target weekly loss range. Current bodyweight × 0.005 is the lower bound (0.5%/week). Current bodyweight × 0.010 is the upper bound (1.0%/week). At 220 lbs, that’s 1.1 to 2.2 lbs/week.
Step 2: Track with a 7-day rolling average. Daily weight swings 2–5 lbs from hydration, sodium, glycogen, and digestive contents. Daily readings are noise. The mean of the last seven morning weigh-ins is the signal. Compare weekly averages for the real trend.
Step 3: If weekly loss consistently exceeds the upper bound, add calories. Protein stays put. Food gets added in this order: protein first to maintain target, then carbohydrates (rice, oats, potatoes), then fats (olive oil, avocado, nut butter). That brings the deficit back into range while keeping the protein lever fully engaged.
Step 4: Recalculate every 4 weeks. As bodyweight drops, the absolute target changes. At 200 lbs, 1.0–2.0 lbs/week. At 180 lbs, 0.9–1.8 lbs/week. Recalculating monthly keeps the floor accurate.
Common Rate Management Mistakes (And How to Correct Them)
Banking fast loss to “make up for” slower weeks ahead. Lean catabolism during aggressive loss isn’t recovered by slowing down later. Tissue lost in weeks 3–8 of rapid loss is gone until you deliberately rebuild it. There’s no catch-up mechanism. Slower and consistent from the start beats aggressive-then-managed.
Not tracking at all and finding the problem on a DEXA. Without weekly tracking and floor adherence, many users don’t realize their rate has run above 1.5%/week until a 12-week scan shows lean loss. By then several pounds are gone. Rate tracking is proactive, not retrospective.
Cutting calories across all macros to fix an aggressive deficit. When loss runs hot, calories come back, but not equally. Protein stays at or above target; the calories come from carbohydrates (timed around training) and fat. Cutting protein to meet a floor is the wrong trade. The reason protein is non-negotiable is the mechanism behind that rule.
Treating the caloric floor as a ceiling. The floor is the minimum, not the target. If appetite allows more on a given day, eating closer to TDEE minus 15% is fine. The floor prevents excessive loss; eating above it doesn’t create a problem.
When does this matter most? Three windows: the first four to six weeks when suppression is strongest, any dose escalation when nausea re-emerges, and any stretch where weight is dropping faster than the rolling average says it should.
The signal I would act on is two consecutive weeks above 1% of bodyweight. Intake comes up, protein first, until the rate returns to range. Waiting for a third week gives the aggressive deficit more time to do damage.
What a Caloric Floor Looks Like in Practice
A caloric floor is a minimum daily intake held regardless of hunger. GLP-1 reliably pushes intake below this without any subjective signal of undereating, so tracking is the mechanism for catching it.
For active men training at least three times weekly, a reasonable starting floor is TDEE minus 15–20%. Estimate TDEE with Mifflin-St Jeor, apply a conservative activity factor, then subtract 15–20% and treat the result as the minimum. The estimate will not be perfect. The 7-day rolling average tells you whether it needs adjustment.
Protein comes first. If 150 g protein is the target (600 calories), the remaining calories up to the floor come from carbohydrates and fats in whatever combination supports training and GI tolerance. Protein shakes in water are the most efficient tool for meeting the floor on low-appetite days.
The goal isn’t to eat more than you want. It’s to keep the deficit within the range that lets the body draw predominantly from fat. GLP-1 is excellent at creating deficit. Your job is to shape it so it works for your body composition, not against it. Rate is the third of three levers, and the framework shows how it interacts with the other two.
Get the Free GLP-1 Starter Framework
Download the free GLP-1 Starter Framework, the three-lever system for losing fat without losing muscle.
The GLP-1 Nutrition Planning Framework covers TDEE estimation, calorie-floor setup, protein targets, meal structure, and the tracker you need to manage rate of loss on suppressed appetite.
FAQ
How fast should you lose weight on GLP-1?
Aim for 0.5–1.0% of bodyweight per week. For a 200-pound man that’s about 1–2 pounds weekly; for a 250-pound man, 1.25–2.5 pounds. Below that range fat loss is slow but lean mass is well protected; above it, the body increasingly draws on muscle for energy. GLP-1 frequently pushes loss past the upper bound in the first weeks, so the rate is something to monitor and manage, not just observe.
Is losing weight too fast on Ozempic bad?
For body composition, yes. Rapid loss, consistently above about 1% of bodyweight per week, means a larger share of what you lose is lean tissue, because fat mobilization has a ceiling and the body covers the rest with muscle protein. It can also worsen fatigue and nutrient shortfalls. Fast scale movement feels like success, but if you care about how you look and perform, the composition of the loss matters more than the speed.
What is a caloric floor on GLP-1?
A caloric floor is a minimum daily intake you commit to regardless of hunger, typically set around your TDEE minus 15–20%. Because GLP-1 removes the hunger signal that would normally stop you from undereating, intake can drift far below what’s healthy without you noticing. The floor is the deliberate correction: you treat hitting it as a daily task, closing any gap with protein shakes and calorie-dense foods on low-appetite days.
How do you slow down weight loss on semaglutide?
Add calories back, in order: protein first to stay at target, then carbohydrates, then fats. Don’t reduce protein. Most often the fix is simply eating up to your caloric floor on days the drug would otherwise leave you well under it. Track a 7-day rolling average of morning weights; if it shows loss consistently above 1% of bodyweight per week, increase intake until the rate returns to the 0.5–1.0% range.
How do you track weight loss rate on GLP-1?
Weigh yourself each morning under the same conditions and average the last seven days. The rolling average filters out daily noise from hydration, sodium, and glycogen. Compare this week’s average to last week’s to get your actual rate, then divide by bodyweight to get the percentage. Recalculate your target range every four weeks as you get lighter, since the absolute pound targets shift down as bodyweight drops.
Nothing on this site constitutes medical advice. I’m not a physician, and this blog documents my own research and experience. Consult a qualified healthcare provider for decisions about medication, dosing, or treatment.
— Ryan Mercer | MetabolicMale.com | ryanmercer@metabolicmale.com
Citations:
Garthe I et al. Effect of two different weight-loss rates on body composition and strength and power-related performance in elite athletes. Int J Sport Nutr Exerc Metab. 2011;21(2):97-104.
Rubino D et al. Effect of Continued Weekly Subcutaneous Semaglutide vs Placebo on Weight Loss Maintenance in Adults With Overweight or Obesity. JAMA. 2021;325:1414-1425.