Progressive Overload in a Caloric Deficit: What to Expect on GLP-1 (And How to Keep Advancing)
TL;DR
- Progressive overload in a caloric deficit on GLP-1 is more achievable than most content about GLP-1 suggests, not just holding lifts, but genuinely getting stronger.
- Neural adaptations like motor unit recruitment, coordination, technique efficiency happen from hard training regardless of energy balance. They don’t need a surplus.
- Dose-escalation weeks will feel like the protocol is failing. Subjective experience is not a reliable signal during that stretch. Performance benchmarks are.
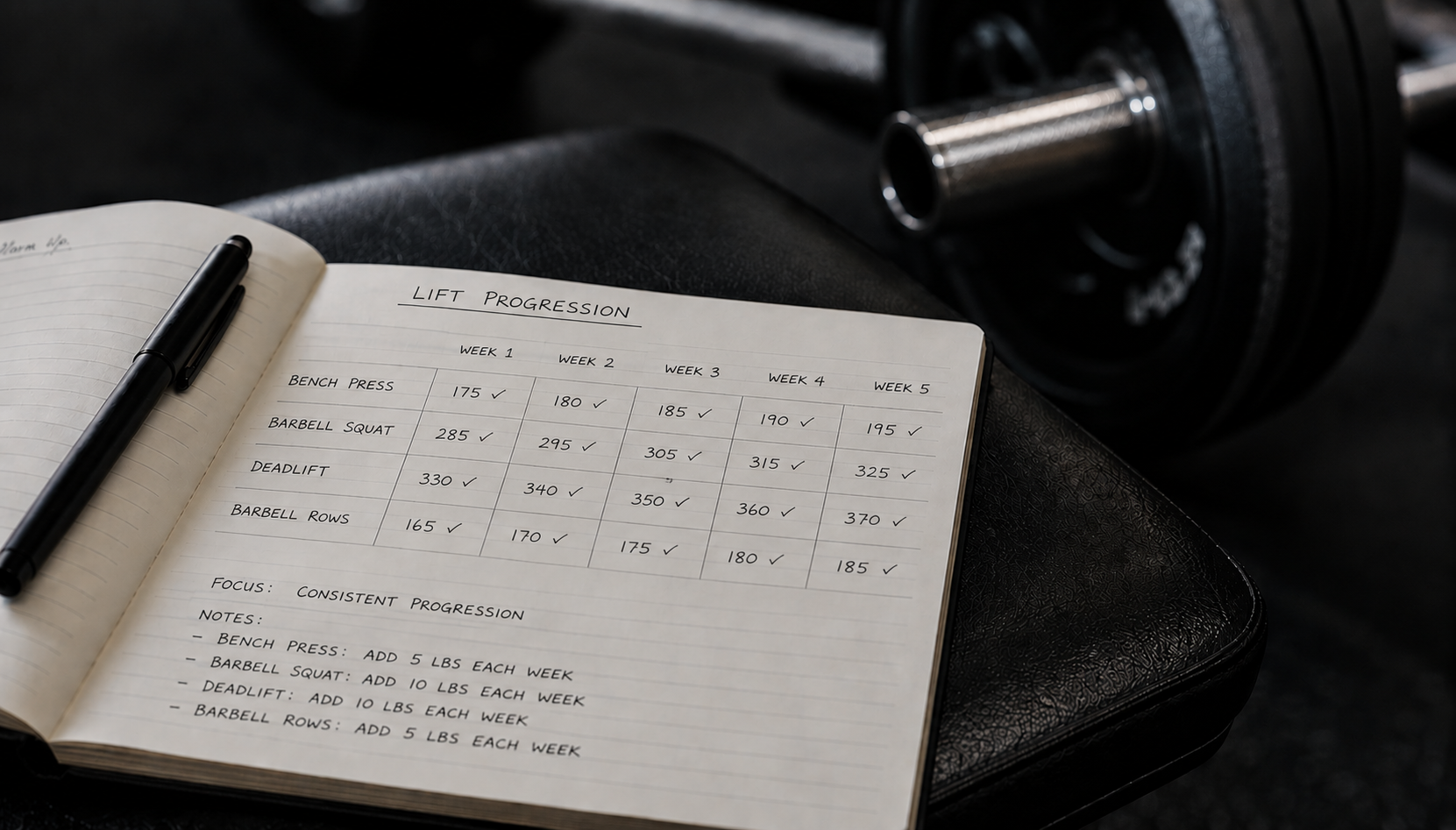
- Ryan’s data: held rep targets through weeks 1–7 while the side effects ran hot, then weights started moving again at week 8. The protocol was working the whole time.
- A stall (loads unchanged, not advancing) during escalation is expected and not a signal to act. A sustained slide (loads declining across sessions) is and the fix is almost always protein or rate of loss, not the program.
Progressive overload in a caloric deficit on GLP-1 is more achievable than most people expect, and considerably more achievable than most GLP-1 content suggests. The standard framing is “expect your lifts to stall.” That undersells what’s actually on the table, gets the psychology wrong, and turns a temporary rough stretch into a permanent expectation.
The honest version is more useful: you can get stronger while losing weight on GLP-1, the dose-escalation period will feel like you aren’t, and the performance data will tell you which one is actually happening.
Why Gaining Strength in a Deficit Is Possible
The gym’s working assumption is that a surplus fuels progress and a deficit stalls it. That’s a reasonable heuristic for maximizing hypertrophy, building meaningful new muscle mass does require an energy surplus over time. But strength gains are not the same thing as hypertrophy gains, and conflating them produces bad advice for GLP-1 users.
Neural adaptations don’t require a caloric surplus
Early and intermediate strength gains come primarily from neural improvements like motor unit recruitment, rate coding, inter-muscular coordination, and technical efficiency.
These adaptations are driven by the mechanical demands of hard training, not by caloric availability. They occur whether you’re eating at maintenance, a surplus, or a deficit. This is why people who return to training after time off regain strength faster than they built it: the neural pathways rebuild quickly, independent of diet.
For most GLP-1 users who are not at an advanced training level, there is still meaningful neural headroom. That headroom gets realized through progressive training regardless of the deficit. It doesn’t require a single extra calorie.
Body recomposition is achievable on a deficit for the right population
Body recomposition (simultaneously losing fat and preserving or gaining lean mass) is achievable in untrained individuals and those with higher body fat percentages, even in a caloric deficit (Barakat et al., Strength Cond J, 2020;42:7-21).
GLP-1 users generally fit that profile: most are not advanced lifters, and most carry enough body fat that the body has stored energy to draw on even when intake is suppressed.
The drug creates the caloric deficit from the outside; the body fills some of the anabolic gap from stored substrate. That’s not a guarantee, but it’s a real mechanism, and it’s why “you can only build muscle in a surplus” is not the whole picture for this population.
Protein-adequate training in a deficit is the operating condition
At 1.6–2.0 g per kg of bodyweight, protein provides the anabolic signal the drug removes by suppressing appetite, the stimulus to synthesize rather than break down muscle tissue (Morton et al., Br J Sports Med, 2018;52:376-384). With protein handled and hard training in place, the deficit is not a ceiling on strength. It is a moderating factor on the rate of progress. Not the same thing.
Download the free GLP-1 Starter Framework, the three-lever system for losing fat without losing muscle.
The Dose-Escalation Reality: Why Subjective Experience Lies
The first two months on semaglutide were not clean. The initial adaptation involved side effects I’d anticipated, and then week five brought the jump to 0.5mg which was harder than the starting dose in ways I hadn’t fully planned for. Some sessions were compromised, some protein targets got missed, and the subjective experience was not one of a protocol running smoothly.
What kept me from adjusting the program during that stretch was the performance data. I was still hitting my rep targets at my working weights. The numbers weren’t advancing, but they weren’t declining either and that meant lean mass was being preserved even when nothing about the experience suggested the protocol was working.
Around week eight, when the side effects settled, the weights started moving again. The strength that followed made the earlier logic feel retroactively obvious: the protocol had been working through the rough stretch all along. The performance benchmarks were the only thing making that visible at the time.
Subjective experience is not a reliable signal during dose escalation. The numbers are.
This is the reason the benchmarks exist not to set a ceiling on what you expect, but to give you an objective read on what’s happening when your subjective experience is untrustworthy. During escalation, the question isn’t “why aren’t my lifts going up” it’s “are they going down?” If they aren’t, hold the program and wait.
What the Benchmarks Actually Tell You
Track one main lift per movement pattern against where it sat at the start of your protocol. The number it returns tells you what to do.
Advancing lifts — the target
If your loads are climbing while your bodyweight drops, you’re gaining strength in a deficit. This is the goal. It means neural adaptations are running ahead of any hypertrophic constraint, protein is handled, and rate of loss isn’t eating into recovery. Let it run.
Stalling lifts — expected during escalation, not a signal to act
If your loads hold steady while bodyweight drops, lean mass is intact. This is the correct outcome during dose escalation or a stretch where protein or energy availability has been imperfect. Hold the program. The advance resumes when the rough stretch passes as it did at week eight. If you feel a lot of fatigue a deload is helpful as well.
Declining lifts — investigate before adjusting anything
A sustained decline across sessions, not a single bad day, but a consistent trend is the signal that something upstream is broken. The cause is almost always one of three things: protein has slipped below target, rate of loss has exceeded what recovery can absorb, or effort per set has drifted soft. Check those in order. The issue is rarely the program structure.
A drop of more than roughly 10% across all key lifts is the red-flag threshold. At that point the fix is upstream: more protein, slower loss, or dialing in effort. Not fewer sets. The decision framework for all of this is in when to reduce training volume on GLP-1.
Progressive Overload Methods That Work in a Caloric Deficit
The temptation when entering a deficit is to immediately switch to “management mode” – substituting rep accumulation and density work for load progression, as if adding weight is no longer on the table. Don’t do this prematurely. If your lifts are advancing, let them advance. Standard weight progression is available in a deficit for most GLP-1 users, especially in the early and intermediate phases of training.
Weight progression — the primary method
Add load when you’ve hit the top of your rep range cleanly across sets. That’s the standard. Don’t skip straight to the alternatives because you’re in a deficit. The alternatives are real tools, but they’re for when the primary method stalls, not for preemptively managing a stall that hasn’t happened.
Double progression — when load progression temporarily stalls
Set a rep range, say 8–12. Hold the load and accumulate reps until you hit the top of the range cleanly across all sets. Then add weight and return to the bottom of the range. This is the correct response to a temporary stall, not a permanent substitute for load progression.
During dose-escalation weeks, double progression is often how you thread the needle: the load doesn’t change, the reps accumulate, and when the escalation settles, the load jumps.
Because of my FAI and labrum issue, I built progression around a 12–20 rep range and double progression instead of chasing heavy low-rep work. That changed the way I read progress during the deficit.
If the load stayed the same but the reps moved up inside the range, the session still advanced. I did not need the bar to get heavier every week to know the muscle was still there.
Density and range-of-motion progression — secondary tools
Doing the same total work in shorter rest periods, or adding range of motion at the same load, are legitimate progression levers that don’t require more weight or more reps.
They’re useful when the primary and double-progression methods are both constrained during a particularly rough week, or at a point where load progression has genuinely stalled for multiple sessions. Not the default; tools available when needed.
The Rate of Loss Variable
How fast you’re losing weight determines how much of your available recovery goes toward adaptation versus deficit management. Losing at roughly 0.7% of bodyweight per week preserved lean mass and allowed strength progression in competitive athletes; 1.4% per week cost lean mass compared to the slower approach (Garthe et al., Int J Sport Nutr Exerc Metab, 2011;21(2):97-104). GLP-1 can push loss rates higher than most users intend, because the appetite suppression runs deeper than a manually maintained deficit typically does.
If your lifts are sliding and protein is handled, check the rate of loss. The full treatment is in how fast you should lose weight on GLP-1. Slowing the rate of loss is often the fastest path to resuming strength gains, faster than any change to the training program.
The Bottom Line
Progressive overload in a caloric deficit on GLP-1 isn’t a consolation prize version of real training. The neural headroom is real, the mechanism is there if protein is handled, and the performance data will tell you what’s happening more reliably than how you feel on a given week. Expect to gain.
Plan for the dose-escalation stretch by trusting the benchmarks rather than the subjective experience. When the rough patch passes, the weights start moving again and the protocol that felt like it was failing was the one that kept everything intact until it did.
For the effort standard that keeps your sets productive through a rough stretch, see why training near failure matters more than set count. The full strength training guide for GLP-1 users puts progressive overload inside the complete protocol.
Download the free GLP-1 Starter Framework, the three-lever system for losing fat without losing muscle.
The GLP-1 Training Protocol ($27) has the full PPL program with both schedule variants, progression rules, GLP-1-specific modifications, and a pre-built Training Tracker spreadsheet.
FAQ
How does progressive overload work in a caloric deficit on GLP-1?
The same way it works at any other time; you progress loads, reps, or density over time with two practical adjustments. First, start with standard weight progression rather than defaulting to management mode; the neural headroom is real and loads can and do advance in a deficit. Second, read the benchmarks rather than subjective experience during dose-escalation weeks. A stall while the side effects run hot is normal; the weights resume moving when the escalation settles, as they did in Ryan’s protocol around week eight.
Can I get stronger while losing weight on semaglutide?
Yes, and for most GLP-1 users who aren’t at an advanced training level, it’s a realistic expectation rather than a lucky exception. Neural adaptations from hard training happen independently of energy balance. Body recomposition, losing fat while preserving or adding lean mass, is achievable in less-trained individuals and those with higher body fat even in a caloric deficit (Barakat et al., 2020). Protein handled at 1.6–2.0 g per kg and consistent hard training are the conditions that make it possible.
Why did my lifts stop moving during dose escalation?
Because dose escalation temporarily stresses the system, side effects compound, appetite drops further, some sessions get compromised. A stall during this stretch is expected and is not a signal that the protocol is broken. What matters is whether loads are declining, not whether they’re advancing. If they’re holding while your bodyweight drops, lean mass is intact and the protocol is working. When the escalation settles, progression typically resumes. Track the numbers rather than the subjective experience.
How do I know if my lifts are stalling or sliding on GLP-1?
A stall means loads are unchanged across several sessions, no advance, but no decline. That’s expected during dose escalation or other rough stretches and doesn’t require action. A slide means loads are dropping consistently across sessions, not explained by a single bad day. A sustained decline of more than roughly 10% across your key lifts is the threshold that warrants investigation check protein first, then rate of loss, then effort per set. The program structure is rarely the issue.
Does losing weight too fast slow strength gains on GLP-1?
Yes. Losing at 1.4% of bodyweight per week cost athletes lean mass relative to 0.7% per week, with strength implications that followed (Garthe et al., 2011). GLP-1 can push loss rates higher than intended because the appetite suppression runs deep. If your lifts are sliding despite handled protein and good effort, the rate of loss is often the culprit.
Nothing on this site constitutes medical advice. I’m not a physician, and this blog documents my own research and experience. Consult a qualified healthcare provider for decisions about medication, dosing, or treatment.
— Ryan Mercer | MetabolicMale.com | ryanmercer@metabolicmale.com
References
- Barakat C, et al. Body recomposition: can trained individuals build muscle and lose fat at the same time? Strength Cond J. 2020;42(5):7-21. https://doi.org/10.1519/SSC.0000000000000584
- Morton RW, et al. A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults. Br J Sports Med. 2018;52(6):376-384. https://doi.org/10.1136/bjsports-2017-097608
- Garthe I, et al. Effect of two different weight-loss rates on body composition and strength and power-related performance in elite athletes. Int J Sport Nutr Exerc Metab. 2011;21(2):97-104. https://doi.org/10.1123/ijsnem.21.2.97